CHAPTER 5 – TREATMENT
As we have read previously, clinically isolated syndrome may develop to multiple sclerosis and because there is no way of determining whether an individual will undergo to develop MS after having an episode of demyelination, making the decision to treat and monitor the ongoing changes very difficult.
Evidence have suggested that the earlier the start of disease modifying agents in the early course of MS the more effective they are. There are numerous studies have indicated that starting disease modifying agents after clinically isolated syndrome delays the onset of MS, but these studies remains controversial.
There have been arguments whether or not to start disease modifying agents after a clinically isolated syndrome. Those who support the start of these agent following diagnosis of CIS cite the results of some clinical trials that shows that these drugs reduce the risk of developing to MS by one third. A “ treat all early “ approach have been proposed as best to ensure all people who would go on to developing MS do receive the treatment .
The other side of this argument have existing evidence for the disease modifying agent in MS shows only modest short term effectiveness in high risk cases of CIS. Treatment is unnecessary for those who would never gone on to developing MS after CIS.
Four large clinical trials have been conducted to determine whether early treatment following an episode of CIS can delay the 2nd clinical episode, and therefore the diagnosis of clinically definite MS
5.1 Controlled High-Risk Subjects Avonex MS Prevention Study (CHAMPS)
The goals of the study are:
Subjects have in this study had experienced a single episode of isolated neurological event suggesting demyelination and had multiple clinically silent MRI lesions, which they represent a high risk for a second neurological attack (definite MS) (40, 41).
The results indicated that AVENOX (interferon beta-1a) had significantly delay the 2nd neurological attack, and MRI finding showed that AVENOX can decrease the volume of brain lesions and as well as fewer lesions . Based on this study, the FDA approved that patients with clinically isolated syndrome with MRI detected brain lesions to receive AVENOX .figure(2).(40)(42)
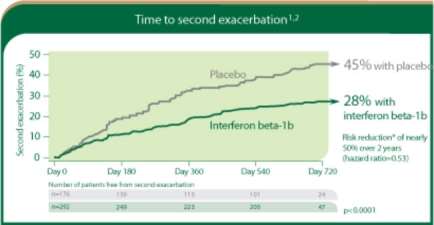
Figure (2): impact of interferon beta following first neurological attack
Source:https://quo.novartis.com/extavia/images/extavia_EFFICACY1_banner.jpg
5.2 Early Treatment Of MS ( ETOMS )
The goals of the study are:
Determine if very low doses of interferon beta 1a (REBIF) delay’s the onset of clinically definite multiple sclerosis in people who experienced only one clinical event but had multiple MRI lesions (43,44).
Results indicated that:
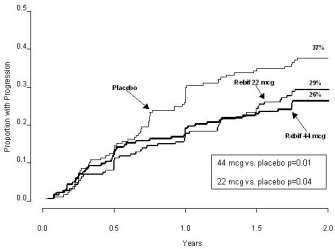
Figure (3 ): compression between the groups receiving REBIF and placebo
Source:http://dailymed.nlm.nih.gov/dailymed/archives/image.cfm?archiveid=100714&type=img&name=rebif-01.jpg
5.3 Betaseron In Newly Emerging MS For Initial Treatment (BENEFIT)
The goals of the study:
Results
The FDA has approved that patients who have experienced CIS and have MRI feature consistent with MS to receive the treatment with Betaseron figure (4).
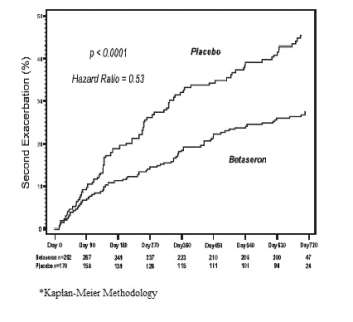
Figure (4): comparison between Betaseron receiving group and placebo group
5.4 The pre-CIS study
Study goals
Determine the period of time it takes for subjects diagnosed with clinically isolated syndrome receiving glatiramer acetate ( Copaxone ) to develop a second attack that would confirm the diagnosis of definite MS.
Results indicated that the group who received glatiramer acetate in comparison with the placebo group, has significantly reduced the risk of developing clinically definite MS.
Based on these results, the FDA has indicated to that individuals who have had first clinical episode and MRI feature consistent with MS to receive copaxone as treatment.
Based on these trials , it have been approved the necessity of starting treatments as soon as possible for clinically isolated syndrome patients and those who have first clinical episode and MRI evidence suggestive of multiple sclerosis (48).
The interferons agents should be used with high cautions by depressed patients or individuals with history of depression because of some evidence indicated that these meds may progress the depression symptoms. In patients with depression the physician should give best possible treatment decision to not worsen the depression episodes and in same time have positive effects in the case of treatment purpose (49).
5.5 Interferon beta medication
Copaxone (glatiramer acetate): in addition to interferon beta drugs, Copaxone has shown to reduce frequency of relapses and the number of new/active lesions on MRI scan. It’s been used in relapsing remitting type of multiple sclerosis. Until the present, the mode of action have not been discovered. Some theories have been suggested but no scientifically proven theory is discovered.(51)
In conclusions, there is no definite treatment of multiple sclerosis or clinically isolated syndrome in the presence of demyelination of the central nerve system. But, reducing the amount of the lesions, frequency of the episodes and prolonging the period of developing MS in high risk patient is the goals we are looking for.
CIS can be difficult to diagnose or to determine whether or not to start the treatment, and the physician may find a hard time to find the best decision in these cases keeping in mind that the sooner the beginning of the treatment the less progressive the disease is (52).
5.6 Prevention
Given to the heterogeneous etiological factors and often idiopathic characteristic of CIS, there are no clear means of prevention exists. In postinfectious patients with CIS, prevention of the infection is the best means of prevention. In acute disseminated encephalomyelitis, almost 70% of cases are associated with infections and 5% (approximately) with vaccination. acute disseminated encephalomyelitis rates are estimated with 1.5 per millions (2 per million) in association with live measles vaccine compared to 1 in 1000 risk of postinfectious ADE with measles infections, suggesting that vaccines may decrease the risk of post infection complications. Unfortunately, vaccines are not available for all bacteria and viruses (53).
Delivering a high-quality product at a reasonable price is not enough anymore.
That’s why we have developed 5 beneficial guarantees that will make your experience with our service enjoyable, easy, and safe.
You have to be 100% sure of the quality of your product to give a money-back guarantee. This describes us perfectly. Make sure that this guarantee is totally transparent.
Read moreEach paper is composed from scratch, according to your instructions. It is then checked by our plagiarism-detection software. There is no gap where plagiarism could squeeze in.
Read moreThanks to our free revisions, there is no way for you to be unsatisfied. We will work on your paper until you are completely happy with the result.
Read moreYour email is safe, as we store it according to international data protection rules. Your bank details are secure, as we use only reliable payment systems.
Read moreBy sending us your money, you buy the service we provide. Check out our terms and conditions if you prefer business talks to be laid out in official language.
Read more